
Infectious Disease Outbreak Response Playbook
Introduction
Outbreaks of infectious disease in animal shelters can dramatically affect lifesaving. In the short term, both infected and exposed animal lives may be at risk depending on the shelter’s available resources. From a long-term perspective, the presence of infectious disease can impact the shelter’s reputation in the community and with partner organizations, and this can limit adoptions or transfer outcomes. The good news is that there are steps that shelters can take not only to prevent outbreaks but also to respond to them using often-limited resources to save the most lives. Perhaps most importantly, shelters don’t have to do it alone – there are experts and resources available to help.
If you’re dealing with an outbreak or if you even suspect one, this playbook is for you. Learn about risk factors, specific diseases, testing strategies, and steps involved in an outbreak response, and then reach out for a consultation if you need more help and we can assist you with your response plans.
Risk Factors
The risk factor of greatest concern for infectious disease outbreaks in animal shelters is population density. Overcrowding in shelters leads to an increased risk of exposure to infectious disease as more animals come into direct or indirect contact with one another. Overcrowding also leads to stress in shelter animals, which suppresses the immune system and therefore makes animals more susceptible to disease. Length of stay is also a risk factor for infectious disease in individual animals. As the average length of stay increases and outcomes do not keep pace with intakes, the shelter’s population density continues to increase.
In overcrowded shelters, staff are often stretched thin and may not strictly adhere to biosecurity and sanitation procedures, resulting in an increased risk of disease transmission. Staff may also not have the time to recognize early, mild signs of infectious disease in individuals, making it possible for those animals to spread disease.
An inadequate vaccination strategy or inappropriate vaccine storage and handling (for those disease which have vaccines available) can also contribute to infectious disease risks. Shelters should store and handle vaccines according to manufacturer instructions and use modified-live vaccines whenever possible. Vaccination schedules should align with current recommended shelter guidelines.
Diseases Commonly Associated with Outbreaks
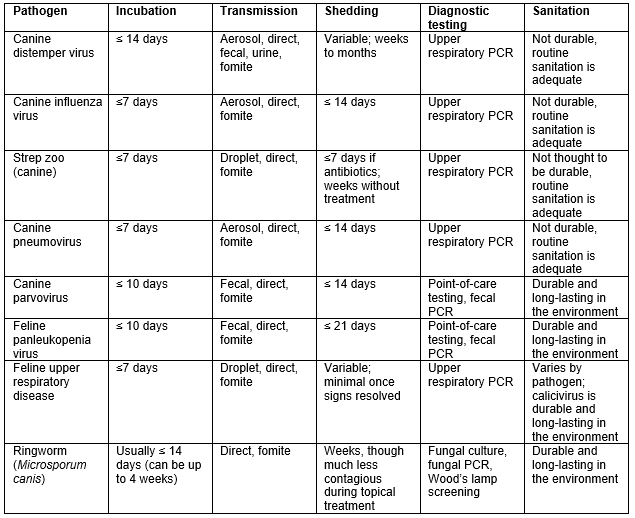
Characteristics of the various specific pathogens are included in the table below. These characteristics will guide the outbreak response, as the period from disease exposure until demonstration of clinical signs (incubation period) varies by pathogen, as does the period of time during which infected animals are contagious (shedding period).
Some pathogens are hardy in the environment, meaning they can remain viable for extended periods of time if disinfection is not performed, and they are extremely long lived in areas that cannot be disinfected (e.g., soil). Canine parvovirus, feline panleukopenia, ringworm, and feline calicivirus all fall into this category.
Diagnostic testing options, discussed in a later section, also vary by pathogen. Transmission of all pathogens can occur through direct contact between animals or objects that indirectly transmit the infective agent between animals (fomites). Common fomites in shelters include cleaning equipment, leashes, toys, food/water dishes, and, most commonly, staff who transmit disease-causing agents on their hands or clothing.
Multiple possible pathogens are associated with feline upper respiratory tract disease and canine infectious respiratory disease (CIRD). Specific canine pathogens of particular clinical significance are outlined separately, given that outbreak response varies by pathogen. For feline respiratory pathogens outside of extremely virulent and uncommon strains, outbreaks are typically handled similarly regardless of the specific pathogen(s).
Steps to Manage an Outbreak
- Identify the problem
- Ask for help
- Diagnose the pathogen
- Create a “clean break” between new animals and sick/exposed
- Communicate to stakeholders
- Isolate sick animals
- Treat and manage individual sick animals
- Quarantine exposed animals
- Perform risk assessment
- Clear animals
- Return to normal operations
Identify the problem
The first step to managing an outbreak is to identify that there is a problem. Isolated cases of infectious disease are unlikely to be completely eliminated from any shelter, so how does a shelter know when they’ve crossed into outbreak territory? Red flags that can indicate a problem include the following:
- More animals affected than is “normal” for the shelter population
- Animals with clinical signs that are more severe than usual
- Notifications of unexpected disease in animals post-adoption or after transfer
A shelter may not be aware that more animals than normal are affected until this number becomes obviously high. Routine disease surveillance, discussed later, is a simple way to identify an increased incidence of disease before the problem is advanced.
Initial immediate steps once there is concern over an outbreak should include halting all animal movement between areas of the shelter and a pause on intake (see more on emergency intake below).
Ask for help
Outbreak management can be complicated, and every outbreak is different. Each shelter has a unique housing facility, different available resources (e.g., financial, staffing, isolation facilities), and varying veterinary capability. Even for shelters that work directly with a veterinarian, consultation with a shelter medicine or infectious disease expert can allow for more efficient use of available resources in order to save the most lives. Some consultation organizations may also be able to offer discounts on testing, offer temporary staffing support for the outbreak response, or offer grant funding to help offset the financial burden.
It is strongly recommended that any shelter experiencing an outbreak reach out for shelter medicine expert consultation.
Find out more about Best Friends’ Shelter Medicine Outreach Program here, and request assistance with an outbreak either through your local strategist or by using this form.
Other assistance programs include:
Diagnose the pathogen
The clinical signs observed in the population will suggest a list of potential pathogens to consider. Diagnostic testing, while resource-intensive, is required to quickly identify exactly which pathogen(s) are involved and to inform the response. Delaying testing can lead to ongoing transmission and an increased number of affected animals.
For canine infectious respiratory disease, a respiratory PCR panel is indicated. Even if a particular agent is suspected, the reality is that no disease can be diagnosed on clinical signs alone and outbreaks that involve multiple pathogens are common, so initial testing should include a full panel. Respiratory PCR is also used to diagnose canine distemper, discussed in detail in this resource.
In outbreaks of feline respiratory disease, while PCR testing is available, it is often not necessary unless a particularly severe strain is noted. Watch this on-demand webinar to learn more about feline respiratory disease management in shelters.
Canine parvovirus can be diagnosed via a kennel-side point-of-care test. These tests can also be used in cases of suspected feline panleukopenia, but performance is not as good, therefore a negative test in a suspicious kitten should not eliminate the disease from the differential list. Fecal PCR testing is available through reference laboratories.
Ringworm is also a cause of outbreaks in shelters and can be diagnosed via fungal cultures or PCR testing. Review this resource on ringworm management for more information.
Not all labs are created equal when it comes to testing; consultation with an outbreak expert can help guide testing. The cheapest lab may not be the most effective – results are not always black and white, and a lower testing cost may be associated with a longer time to receive results. This can mean ongoing transmission back at the shelter, which can ultimately prolong the outbreak.
For pets who die or are euthanized, necropsy can be an invaluable tool. It is recommended that this be performed by a veterinarian familiar with shelter pathogens or by a pathologist so that appropriate testing is performed. Respiratory PCR can be used on lung samples in cases of pneumonia, and culture of lung or organ tissue may provide useful information.
Create a clean break
In order to stop the cycle of transmission, new animals and any unexposed animals must be kept completely separate from the sick and exposed population.
For many of the common shelter pathogens, animals can be infectious BEFORE they begin to demonstrate clinical signs of disease. This means that healthy-appearing animals can transmit infectious disease, and in most cases, it’s impossible to know which animals are infectious without testing. If a shelter continues to admit new animals to the population, these infectious (but asymptomatic) animals can transmit disease, and the cycle will continue.
One strategy to create clean break is to restrict shelter intake to those cases for which it is absolutely necessary (e.g., emergency intake). Animals included in this category include:
- Severely injured or ill animals
- Animals who pose an immediate threat to public health or safety (e.g., dangerous dogs, rabies-suspect animals)
- Animals who are in danger (e.g., uncontained at a dangerous intersection, in a cruelty situation)
Every effort should be made to divert healthy animals and postpone owner surrenders. Various ways to achieve this include:
- Diverting new intakes to an off-site location designated for this purpose
- Diverting new intakes to partner shelter organizations or rescues
- Recruiting finders of stray animals as temporary foster caregivers
- Supplying resources to owners needing to relinquish so that doing so may be postponed or avoided
A common response from open-intake shelters is that they cannot restrict intake because they are open admission and/or are contractually obligated to take animals. The reality is that continuing to accept animals into a situation with an identified outbreak puts them at risk of contracting serious and potentially fatal infectious disease. Sheltering organizations do a disservice not only to individual pets but to the entire community if they continue to accept animals into outbreak situations, as this only perpetuates the disease and may expose stray animals and lost pets. If an aggressive outbreak response is mounted, including restriction of intake, shelter operations will return to normal much more rapidly than if intake is allowed to continue, as the cycle of transmission will continue unabated.
A template for communicating about an outbreak and implementing emergency intake practices can be found here; here are some examples of communications used by shelters experiencing outbreaks.
A small number of animals (e.g., emergency intakes) will likely still need to come into the shelter’s care and a place should be designated for these animals. This could be an off-site location, foster care, or a designated area of the shelter. Extreme caution must be used if vulnerable animals are kept on site so as not to lead to continued disease transmission. If disease transmission occurs, a new solution must be found.
Communicate to stakeholders
In addition to communication to the community regarding emergency intake, other stakeholders should be notified of the situation. Consider proactive communication to the following:
- Transfer partners which have recently received animals who may have been exposed
- Recent adopters of animals who may have been exposed
- Other local shelters, if community transmission of the pathogen is suspected
Communication to the public can include a call to action, depending on the needs of the shelter. Examples include:
- Request for temporary foster homes for either new intakes (unexposed pets) or for known exposed animals (restrictions on other pets in the home will likely be necessary and will differ based on pathogen)
- Plea for adoptions to reduce the population in the shelter (similar restrictions on other pets may apply)
- If only one species is affected, pleas for foster/adoption of healthy species so that more resources (staff and space) can be devoted to the outbreak response
- Donations to assist with the response, including treatment of sick pets
Shelters may fear community backlash or resistance from transfer partners to receiving pets once an outbreak is publicly declared. Transparency, however, will pay off in the long run. Shelters should be honest about not only their challenges, but also about their responsible approach to dealing with the problem. This will ultimately increase their credibility with the community and transfer partners.
Isolate sick animals
While apparently healthy animals may be contagious, the greatest source of transmission is those animals who are showing clinical signs of illness. For this reason, they must be isolated from the rest of the population and this isolation should occur immediately after signs are noted. Strict biosecurity measures must be in place to prevent transmission of disease from this sick population to the uninfected population.
Ideally, a separate building or facility should be utilized as an isolation ward. If this is not possible, a room can be designated (or a non-animal room equipped with temporary housing). For those shelters with only a single area for housing, a section or row can be sectioned off using a tarp. While shared ventilation is not ideal, the tarps function as a physical barrier and will signal to staff the transition between populations. Lack of a separate ventilation system is NOT a valid reason for neglecting to isolate sick pets. Drainage patterns may be important for some pathogens and can be a source of cross-contamination. The sick population should be situated so that pathogens do not drain into the healthy areas.
If sick animals cannot be isolated appropriately and no alternative housing can be identified, the shelter must consider humane euthanasia of those pets in order to stop continuous transmission of disease. All live outcome options and alternative housing must be explored prior to making this decision. Even if a broader euthanasia approach is necessary, shelters are encouraged to seek live outcomes for individual animals (e.g., transfer to staff willing to foster exposed or sick pets, risk-tolerant rescues, organizations experienced with the disease).
Treat and manage individual sick animals
While in isolation, individual animals should be treated by medical staff under the supervision of a veterinarian. Various treatment protocols exist to aid in the efficient provision of care for most diseases, and a veterinarian may not need to be directly involved in evaluation of all straightforward cases (where this is allowed by law).
The Association of Shelter Veterinarians supports the use of protocols to manage common shelter medical conditions. Here are examples of treatment protocols:
- Canine distemper treatment
- Canine parvo treatment
- Ringworm protocol and in-house culture protocol
- University of Florida disease management resources (includes many diseases)
A veterinarian must be consulted on all cases of severe disease and for all non-routine cases. Ideally, a veterinarian will be able to examine all sick animals (as well as monitor the healthy and exposed populations).
For more serious, potentially life-threatening diseases, it may make sense for shelter leadership – under the direction of a veterinarian familiar with the disease – to determine end points that warrant euthanasia. This demonstrates transparency to staff and ultimately allows the shelter to save the most lives possible through judicious use of resources.
Quarantine exposed animals
Any vulnerable pets who have been exposed to the disease must be quarantined and monitored closely for signs of infectious disease for a period of time equal to the maximum incubation period for the pathogen of concern. Any time a new animal breaks with disease, that quarantine clock must be reset, as a new potential exposure has occurred.
It is possible that quarantine restrictions may be relaxed over time for vaccine-preventable diseases in adult dogs (primarily canine distemper). However, this should only be done when a shelter veterinarian can verify that animals with previous vaccinations are low-risk. Vaccinations do not take effect immediately; even vaccinated animals, if exposed in the days immediately following the vaccine, will not have had time to mount a full immune response and thus can still become infected. Titer testing can help to provide additional information (see Perform risk assessment).
Perform risk assessment
Depending on the pathogen, not all animals in the shelter may be susceptible to the pathogen of concern. Canine parvovirus is almost exclusively a disease of puppies under 6 to 12 months, though isolated outbreaks affecting older populations have occurred. Adults, particularly those with a vaccine history at the time of exposure, can often be considered low-risk and may be eligible for transfer or adoption without restrictions. Feline panleukopenia virus has been known to affect adult cats in certain geographic regions and so caution should be used when designating adult cats as low-risk. Titer testing can provide useful information.
A large percentage of adult dogs entering shelters do not have immunity to canine distemper upon intake, and many dogs need 2 vaccines and more than 2 weeks in the shelter to achieve a full immune response to vaccination. Exposure at any point prior to that 14-day length of stay may result in infection. Titer testing can help identify immune individuals but must be paired with PCR testing to ensure the titer is not from active infection.
Titer testing looks for the presence of antibodies, the immune system component which fights the disease of concern. In cases of diseases for which we vaccinate, vaccination induces the production of antibodies. Antibodies may also come from infection, however, and without a negative diagnostic test, it is impossible to interpret a positive (or “protective”) titer as coming from antibody (indicating immunity) versus active infection in a pet who is not yet showing clinical signs.
There are other pathogens for which either vaccines are not available (many canine and feline infectious respiratory pathogens), for which vaccination is uncommon (canine influenza), or for which vaccination does not provide full protection (e.g., feline calicivirus, feline herpesvirus, Bordetella). In these situations, all animals are considered potentially at risk of becoming infected.
Clear animals
The strategy for clearing exposed animals is based on the quarantine clock. Once an incubation period has passed with no infection (as determined by presence of clinical signs and/or testing), these pets can be cleared. Disclosure to adopters or receiving partners is still prudent, though, as we can never completely eliminate the risk of transmission.
Clearing infected pets will be dependent on the pathogen of concern. Parvovirus and panleukopenia are shed for a predictable period of time following infection and so pets can be cleared after 14 days in the case of canine parvo and 21 days in the case of panleukopenia. Snap testing is sometimes used to clear animals sooner, but is not sensitive later in infection, particularly for panleukopenia. Low levels of shedding may not be clinically relevant if these animals are housed with other vulnerable pets, and decisions should be made with the individual shelter situation in mind.
For most causes of canine and feline infectious respiratory disease, animals are minimally contagious after resolution of clinical signs and pose a low risk (though perhaps not zero!) to other pets. Canine distemper is the exception, although it is unlikely to be transmitted via aerosols if no coughing is observed (fomite transmission, fecal, urine, and direct transmission are still of concern).
Strep zoo is also an exception; animals treated prophylactically with antibiotics can be considered non-contagious after 7 days. Any treatment with antibiotics should be conducted under the supervision of a veterinarian and routine use of prophylactic antibiotics is NOT recommended, even in outbreak situations (Strep zoo outbreaks remain a rare exception to this principle due to rapid progression of fatal disease, within hours in some cases, before clinical signs can be identified).
Return to normal operations
When is an outbreak considered resolved? Typically, for full resolution to be declared, at least 2 incubation periods must have passed with no new cases of disease. As this period is approached, however, a gradual and staged return to normal operations should be considered.
For some pathogens with widespread shelter transmission, like pneumovirus or canine influenza, if testing to clear animals is not performed, animals may be held for the contagious period and then released either based on absence of clinical signs or on maximum shedding period. This should be done under the guidance of an infectious disease expert to prevent spread to the community after release.
Regardless of the state of the shelter, a gradual return to normal operations may be beneficial to allow staff the time to recover from what is often a challenging period. A staged opening might mean initially reopening intake from animal services officers and not the general public, followed by resuming owner surrenders and intake of over-the-counter stray and lost pets at a later date. Clear communication to all stakeholders is necessary.
Sanitation and Biosecurity
Sanitation
A disinfectant product that is effective against all pathogens of concern is recommended. Despite label claims, the quaternary ammonium compounds are not reliably effective against hardier pathogens like parvovirus. This resource from the American Society for the Prevention of Cruelty to Animals is updated regularly and summarizes the various product classes. Rescue, Wysiwash, and Trifectant are effective choices for parvo, panleukopenia, ringworm, and calicivirus.
Using the appropriate dilution with exact measurement or a commercially available dilution system is required. Approximating the dilution is not sufficient and products may not be effective at alternative dilutions. Contact time, as specified in the resource, must also be adhered to; this contact time means wet product that is maintaining contact with the surface. Even “one-step” products are ineffective if caked-on debris is preventing the solution from contacting the surface. Therefore, sanitation ALWAYS includes 2 steps: cleaning followed by disinfection.
See the Best Friends Operational Playbook on Disease Control - Role of Sanitation.
For animals remaining in the same primary enclosure without excess contamination, spot-cleaning is appropriate and will reduce stress on individual animals. Regular deep cleaning will reduce pathogen loads in the environment, however, and should be considered on a more frequent basis in areas with sick animals as compared to the general population. Multiple cycles of deep cleaning may be appropriate when placing a new, healthy animal into a kennel where a sick pet was residing. These additional cycles do not actually provide additional disinfection, but if there are potential cracks, crevices, or places where disinfectant may not reliably reach, multiple cycles will ensure that at least once full contact time is achieved.
Biosecurity
Staff adherence to biosecurity measures is paramount. Ideally, separate staff are designated for each area of the shelter. If separate staffing is not possible, then the order of cleaning should be as follows:
- Healthy, unexposed, most vulnerable (puppies, kittens)
- Healthy, unexposed, least vulnerable (adults)
- Quarantine areas - Healthy, exposed, most vulnerable (puppies, kittens)
- Quarantine areas - Healthy, exposed, least vulnerable (adults)
- Isolation areas – sick animals (known to be or likely to be contagious)
Color coding rooms/areas based on level of disease can be helpful. Staff and equipment should then be identified with visual indicators based on those colors. n example frequently employed in shelters is a stoplight system: healthy/unexposed or cleared animals are designated green, exposed but asymptomatic animals under quarantine are yellow, and any obviously sick pets are red (isolation). This system can be modified under the guidance of a shelter medicine expert and based on the pathogen and the shelter’s ability to treat a particular disease.
Personal protective equipment (PPE) should be used in any quarantine or isolation space and should not leave the room. PPE may also be indicated for use with all pets in the shelter during outbreaks or in shelters that frequently deal with infectious disease. Dedicated equipment and supplies should never be removed from an isolation/quarantine room. Commercially available isolation gowns do not cover the entire body and are inadequate for dogs. Instead, full-body coveralls or dedicated scrubs (purchase extra-large fabric scrubs that can be worn over regular clothing, then washed) are recommended. Dedicated footwear is preferred over shoe covers that are often flimsy and do not cover the entire shoe. Footbaths are inadequate as contact time is not achieved by walking through them and organic material collects and can harbor pathogens.
Even within a particular room or area, it is important for staff to change PPE between individual animals so that any contagious animals still in their incubation period do not transmit disease via staff and fomites. While this can seem tedious and labor-intensive, any reduction in transmission will ultimately mean a faster resolution of the outbreak and more lives saved. PPE must also be donned and doffed in a manner that does not contaminate the individual’s clothing.
Prevention
Vaccination
Vaccination using a modified live vaccine immediately upon intake (or prior to intake) and stringently following with an additional dose of vaccine 2 weeks later gives the greatest opportunity for individual animals to develop immunity. Vaccination should continue every 2 weeks until 18 to 20 weeks of age for juvenile animals.
Reduce overcrowding
Overcrowding is a known risk factor for infectious disease in shelters, as it contributes to an increased risk of exposure and increased stress, which suppresses the immune system. Overcrowding also impacts staff ability to properly adhere to sanitation and biosecurity protocols.
Reduce transmission with biosecurity
Biosecurity measures, similar to those outlined previously for known sick or exposed populations, may be warranted with all animals or, at a minimum, with vulnerable populations (e.g., juvenile animals, new intakes without known disease or vaccination history).
Reduce length of stay and exposure
Fast-tracking the most vulnerable animals out of the shelter environment (through adoption or foster) will reduce their risk of disease. Even after multiple vaccines, puppies and kittens have variable immunity due to the presence of maternal antibodies that can interfere with vaccination, and so we cannot consider them reliably protected until after 4 to 5 months of age.
Reducing animal movement in the shelter will reduce potential disease exposure points and reduce stress that can also increase the risk of disease. Each time an animal changes location, staff may transmit disease or become contaminated. The new enclosure is also a new potential source of contamination, and the animal is exposed to new neighbors, thereby increasing the potential for disease exposure. Even healthy-appearing animals may be contagious while still in their incubation period.
Rapid identification and isolation
The animals most likely to transmit infectious disease are those who are actively demonstrating clinical signs, as they are typically shedding large amounts of pathogen into the environment. In the case of respiratory disease, they can transmit these pathogens long distances in droplets or aerosols (up to 20 feet). These animals must be identified rapidly and moved to isolation.
All staff, animal services officers, and volunteers should be trained in the basic recognition of infectious disease and should know what steps to take when it is identified (e.g., who to notify and how to notify them if they are not themselves empowered to isolate the pet). Staff should know the process for moving an animal to isolation and a time frame within which this movement happens should be established (within x number of hours or minutes, if possible). Movement should never be postponed until the next day as this unnecessarily exposes many animals for a prolonged period and virtually ensures susceptible, exposed animals will become infected.
Daily population rounds, a physical walkthrough of the entire shelter performed by key medical and operations staff, can help to rapidly identify animals with signs of contagious disease, though all staff at the shelter should be trained in disease identification. For shelters not practicing daily rounds, a walkthrough specifically for disease identification by a trained staff person may be a more feasible solution, though all shelters are encouraged to develop a process for daily rounds, regardless of staffing numbers or intake size.
Disease surveillance
Shelters should routinely track incidence of infectious disease in their populations so that upticks in disease can be identified. Any increase in disease warrants an investigation, as does an increase in the severity of individual cases.
An example of this might be a shelter where canine distemper is endemic in the community. All cases of CIRD are isolated immediately, and either all cases or some percentage of cases are routinely monitored with a canine distemper virus PCR to distinguish between distemper and other causes of CIRD. In other shelters where distemper is of less concern, isolation is still recommended, but routine respiratory PCR testing may not be indicated except in more severe individual cases.
Resources, References, and Links
Best Friends Shelter Medicine Outreach Program
Best Friends Webinar on Disease Prevention in Shelters
University of Florida: Disease Outbreak Management in Shelters
University of Florida: Disease Prevention and Response in Animal Shelters
Association of Shelter Veterinarians Position Statement on Veterinary Supervision in Animal Shelters
Association of Shelter Veterinarians Guidelines for Standards of Care in Animal Shelters and checklist of key statements
Association of Shelter Veterinarians Guidelines for Standards of Care in Animal Shelters
Janke KJ, Jacobson LS, Giacinti JA, Weese JS. Fecal viral DNA shedding following clinical panleukopenia virus infection in shelter kittens: a prospective, observational study. J Feline Med Surg. 2022 Apr;24(4):337-343. doi: 10.1177/1098612X211023056. Epub 2021 Jun 25. PMID: 34170191; PMCID: PMC8961250
Examples of outbreak communications:
Examples of templates:
- City of El Paso Animal Services: Frequently Asked Questions Regarding Our Response to the Current Upper Respiratory Outbreak
- City of El Paso Animal Services Press Release: Animal Services Responds to Strep Zoo and Distemper Outbreak
- Riverside County Department of Animal Services: Shelter Responds to Strep Zoo Outbreak