
Canine Distemper Playbook
Introduction
Canine distemper is a highly contagious viral disease that can affect dogs of all ages, and it is endemic in many parts of the country. Distemper is not a death sentence, however — not for individual dogs, and certainly not for all the dogs in the shelter. This playbook gives an overview of canine distemper, to help you understand the implications of the disease in shelters, and to teach you how to approach prevention, treatment and even transport in the shelter environment.
Disclaimer: The information provided in this article is for educational purposes only and is not meant to replace or substitute for advice from a licensed veterinarian regarding veterinary medical care.
Background
Transmission
Transmission occurs when virus particles are shed from an infected dog, typically in respiratory secretions, but also in urine, vomit or feces. Virus can become aerosolized into a mist when a dog coughs or sneezes and can travel as far as 20 feet from the infected dog.
Distemper virus survives for only a few hours at room temperature, but this is long enough to include fomite transmission (transmission of particles on inanimate objects like cleaning supplies, medical equipment and staff clothing or even on hands) as an important mode of transmission in the shelter setting. The incubation period (the period of time from when a dog is exposed to the virus to when he begins showing clinical signs) is most commonly 10-14 days, though it can be as long as a month.
Clinical signs
The most common clinical signs include upper respiratory signs (cough, nasal discharge, conjunctivitis) and gastrointestinal signs (vomiting, diarrhea, decreased appetite). In some cases, the upper respiratory signs may progress to lower respiratory disease (pneumonia). About 10% of dogs infected develop neurological signs, which can range from mild tremors to severe seizures.
The virus can infect any (or all) body systems, and clinical signs may reflect this. Less commonly observed signs include ocular disease, skin lesions and/or urinary/kidney disease. Finally, many dogs may not demonstrate any clinical signs of disease and appear asymptomatic; they are identified only through diagnostic testing.
Diagnosis
Dogs with distemper infection experiencing only upper respiratory signs cannot be distinguished from dogs with other causes of canine infectious respiratory disease (CIRD, also known as kennel cough), such as Bordetella, by clinical signs alone. If distemper is suspected or possible, respiratory swab collection and PCR (polymerase chain reaction) testing is recommended. This testing looks for the presence of viral DNA in samples obtained from the dog’s nose, conjunctiva and pharynx (throat). Quantitative testing provides not only a positive or negative result, but also a viral count that can be useful for interpretation and disease tracking in individual dogs. Here are some helpful resources regarding sample collection:
- How to collect a sample for respiratory PCR – document from University of Florida
- How to collect a sample for respiratory PCR – video from University of Florida
If a modified live vaccine is used, this may lead to positive results on a distemper PCR test for 1-2 weeks after vaccination (this occurs in about 20% of healthy dogs). If you suspect this, we recommend treating the dog as if he is infected (as a precaution) and retesting in 1-2 weeks. If vaccine-induced, the viral count will decrease dramatically and go to zero (negative) within that time frame of 1–2 weeks.
Prevention
While the percentage will vary among shelters and regions, studies have shown that up to 60% of dogs entering shelters do not have adequate immunity to canine distemper virus. If exposed to the virus, they will likely become infected. This percentage may increase to above 80% in young dogs (under one year of age).
We recommend that all dogs be vaccinated immediately upon intake to the shelter with a modified live vaccine for distemper (typically given in a combination vaccine that protects against other common pathogens like parvovirus). Recombinant vaccines are available for distemper but are not recommended in high-risk settings, so shelters should use modified live vaccines whenever possible.
After vaccine administration, a protective immune response takes time to develop. Most dogs will not develop full immunity until more than two weeks after initial vaccination, when they are given a second dose of vaccine. Vaccination schedules should align with shelter vaccination guidelines.
Vaccinating with a modified-live distemper vaccine immediately upon intake AND stringently following with a booster vaccine 14 days later is key to preventing canine distemper transmission in the shelter setting.
Treatment of individual dogs
All treatment must be performed under the guidance of a licensed veterinarian. Treatment of dogs with canine distemper is supportive in nature; there is no effective treatment that directly combats the virus. Dogs with distemper are often treated similarly to kennel cough dogs when upper respiratory signs develop (most commonly with doxycycline), although antibiotics are not indicated in all cases of kennel cough.
For more serious signs, distemper dogs can be treated with gastrointestinal medications (for vomiting or diarrhea), fluid therapy to maintain hydration, and/or specific medications aimed at neurological signs. For dogs who develop pneumonia, broad spectrum antibiotics are indicated, and severe cases may require oxygen supplementation.
For the 10% of dogs who develop neurological signs, these signs may resolve over time or they may be permanent. If signs are mild and don't affect quality of life, then many
dogs live with them without a problem. If signs are severe (frequent or long-duration seizures that do not respond to treatment, or tremors that are adversely affecting the dog’s ability to eat, drink and ambulate), humane euthanasia should be considered.
Survival rates for adult dogs are high with treatment (greater than 90%), and many adult dogs demonstrate only mild signs. If infected dogs can be housed in a manner that does not put the rest of the population at risk, shelters should absolutely explore some degree of treatment, even if only for more mild cases. Survival in puppies is more variable, and they become severely affected more commonly, though many can be treated successfully and survive. For more information, see the treatment protocols linked below.
Prevention and Management in the Shelter Setting
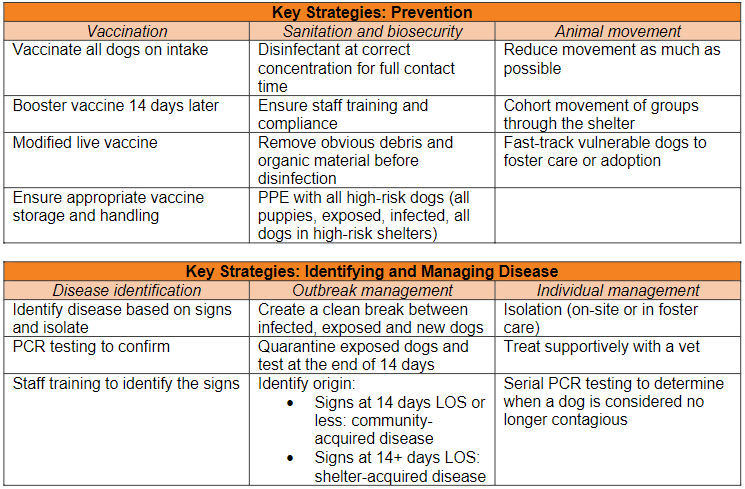
The key components of shelter management include:
- Vaccination on intake with a modified live vaccine
- Immediate isolation of potentially infected dogs
- Limiting dog movement and reducing overcrowding
- Fast-tracking or foster homes for the most vulnerable dogs
- Sanitation
Prevention
Vaccination has been addressed above. Common pitfalls in shelters include missed or delayed booster vaccination or inappropriate vaccine storage and handling (reconstituted too soon before administration, not maintained at the appropriate temperature).
Because distemper’s primary modes of transmission are through contact with respiratory particles (that can travel up to 20 feet from the infected dog) and through fomite transmission, shelter management strategies aimed at reducing spread are imperative to keep infection isolated to one or a few dogs, rather than developing into an outbreak situation. Any dogs with consistent clinical signs should be isolated from the general population immediately.
Infected dogs may begin shedding virus up to three days before clinical signs develop, and some dogs may have completely asymptomatic infections. While these dogs do not typically shed the large amounts of virus that more clinically affected dogs do, they still pose a transmission risk. With each move a dog experiences from kennel to kennel, he potentially exposes an entirely new set of neighbors to the virus, since any dog within a 20-foot radius may become exposed.
Limiting dog movement will reduce the exposure of potentially affected dogs to vulnerable dogs, and it will also keep staff from becoming contaminated during animal handling. For shelters that use a common space for intake procedures, this area or room is often a source of cross-contamination if it’s not adequately disinfected between every new animal. Animal control vehicles are another potential source of exposure, if dogs from multiple locations are transported together.
Appropriate disinfection is key to preventing the spread of disease. Distemper is inactivated by most common disinfectants used in shelter settings, but the presence of organic material may inactivate many of these products. Care should be taken to remove any solid material (feces, food) prior to the disinfection stage, and the manufacturer’s instructions should be followed regarding necessary contact time for disinfection. Disinfection procedures should extend beyond shelter housing and must include any areas where animals are handled, examined or treated, as well as animal control vehicles.
Management of disease, once it is identified
Prompt isolation of infected (or potentially infected) dogs is paramount. Exposed dogs should also be kept separate from unexposed dogs. Exposed dogs may be assessed based on their risk (age, vaccination status) to determine next steps. If they are vulnerable, they may be tested at the end of the typical incubation period to determine infection status. Individual dogs should be treated based on clinical signs (as outlined above), as long as they can be housed in a place where they do not pose a transmission risk, either in isolation in the shelter or a foster home.
There is often a desire to interpret positive test results as vaccine-induced. In the face of an outbreak or in the presence of confirmed disease, every positive result should be handled as true infection until proven otherwise. Often, these dogs have low viral counts, and laboratory testing ranges may indicate that the count is consistent with vaccination. Low viral counts also occur, though, in early and late infection and throughout mild infection, so results must be interpreted cautiously. Serial testing (1-2 weeks later) will help to determine if the infection is real or if the result is vaccine-induced.
Although infected dogs may test positive on serial PCR tests for prolonged periods (weeks to months), recent research has found that these dogs are unlikely to be contagious for this entire duration. This new research has allowed the shortening of isolation periods for recovering dogs, allowing more shelters to successfully treat infected dogs without risking transmission over long periods. Commonly, dogs must remain isolated for only two to four weeks, rather than weeks or months, as was commonly practiced prior to this new research.
To determine that a dog is no longer infectious, serial quantitative PCR testing should be conducted. Once the dog’s viral count is steadily declining, they can be deemed no longer contagious and no longer need to be isolated from other vulnerable dogs. This treatment protocol outlines the procedure in detail, and you can reach out to our National Shelter Medicine team for guidance on testing and result interpretation.
Even with shortened isolation periods for infected dogs, two to four weeks in the shelter may still pose challenges for the individual dog’s welfare and for the shelter. It is safe to house distemper-positive dogs in foster care either as the only dog or with adult, fully vaccinated dogs. This is preferable to extended in-shelter stays, where they may risk exposing other dogs and where their overall welfare (particularly mental) may be compromised.
When distemper is identified in a shelter population, it is important to determine whether that infection was likely acquired BEFORE entry to the shelter or if transmission occurred during the dog’s shelter stay. In practice, 14 days is often used as the guideline. Dogs who develop signs prior to a 14-day length of stay are likely to have acquired the infection in the community; dogs who develop signs with a 14-day or longer length of stay likely acquired the infection in the shelter.
Community reservoirs of the disease may exist and monitoring the locations where these dogs come from can guide targeted community vaccination programs. For in-shelter transmission, leadership must carefully evaluate current protocols for sanitation, animal movement, vaccination (including storage and handling) and staff compliance. If possible, determine when a dog was exposed and which additional dogs might have been exposed.
Overcrowding in shelters contributes to the spread of disease, including canine distemper. Operating the shelter within its capacity for care (staffing, housing and outcome-driven capacity) will reduce infectious disease spread. For shelters struggling with canine distemper, a holistic evaluation of all shelter operations is often indicated.
Lifesaving Programs
Foster care
For shelters dealing with canine distemper, foster care programs can be used in several ways. Clinically recovered dogs who are still contagious (or even mild cases still undergoing basic treatment) may be housed in foster care until they test negative. Public education is often needed to recruit foster volunteers who are comfortable taking on a distemper-positive dog, but many shelters have successfully implemented this type of foster programming.
Foster care is also ideal for the most vulnerable population — young puppies or nursing mothers with puppies — to reduce their risk of exposure. Housing them in foster care removes them from the high-risk shelter environment and provides better socialization during a critical period.
Transport
Many of the shelters that most commonly deal with canine distemper are also some of the shelters that continue to have high intake numbers and face ongoing challenges on their path to reaching and sustaining no-kill. Because of that, transport is often a vital part of the lifesaving equation. Transporting dogs from regions where distemper is endemic can be done safely, if appropriate precautions are taken.
Various models exist, and some effective strategies include:
- Quarantine of dogs, either at the receiving shelter or before transport, and ideally in foster care
- Reducing the number of source shelters placing dogs on a single transport vehicle (to limit new exposures, in the same way that limiting in-shelter movement reduces exposure)
- Screening of dogs with PCR testing either upon arrival or before transport
- Partnerships between receiving and sending shelters that provide financial resources and mentorship to implement prevention strategies (such as vaccination on intake)
Summary


Sample Procedures, Program Documents and Additional Resources
- Recovering distemper dog handout (discusses PCR positive status does not necessarily indicate contagious risk)
- Updated guidance from the University of Wisconsin
- Best Friends operational playbook on sanitation
- Distemper testing and treatment protocol (Best Friends)
- SDHS Distemper Protocol
- SDHS Distemper Agreement for Foster Homes
- SDHS Distemper Fact Sheet for Foster Homes
- Vaccine storage and handling (ASPCApro)
Updated May 2024
If you found this playbook helpful, check out our full catalog of handbooks, manuals, and playbooks.