
Heartworm Disease Management Playbook
Introduction
While heartworm disease has been identified in all 50 U.S. states, its prevalence is variable. In areas of lower prevalence, shelters, rescue groups and veterinarians are rarely faced with heartworm management, so this disease may seem daunting. However, shelters in the South struggle daily with heartworm, as this disease affects 20% or more of dogs entering shelters in that part of the country. Transport of heartworm-positive dogs to receiving partners willing to take on the challenge can open vital lifesaving capacity in the shelters most in need.
This guide provides an overview of heartworm disease management, from the point of case selection (even as early as when the dog still resides at a sending shelter) all the way through treatment. The purpose is to walk organizations through the process of transporting and treating heartworm-positive dogs safely and efficiently, so that more lives can be saved.
Program Overview
The American Heartworm Society (AHS) recommends the use of doxycycline and heartworm prevention, followed by a three-injection melarsomine protocol for all dogs, regardless of severity of infection. This protocol has shown better efficacy than alternatives (including two-injection melarsomine protocols). While the two-injection protocol may be appropriate in some shelter settings, choosing a three-injection approach is becoming more common across treatment settings. Should shelters choose any alternative protocol, they should understand the risks and benefits associated with that alternative.
The following treatment outline includes the AHS-recommended protocol but skips the pre-treatment diagnostic testing regimen that is commonly recommended by veterinarians. The small risk of underlying disease or illness that may affect treatment is mitigated through conservative patient selection (i.e., choosing lower-risk dogs for treatment), and by foregoing extensive diagnostic testing, time, staff and financial resources can be extended to save more lives. For severe or advanced cases of heartworm infection, diagnostic testing prior to treatment is strongly recommended.
Program Composition
Case selection
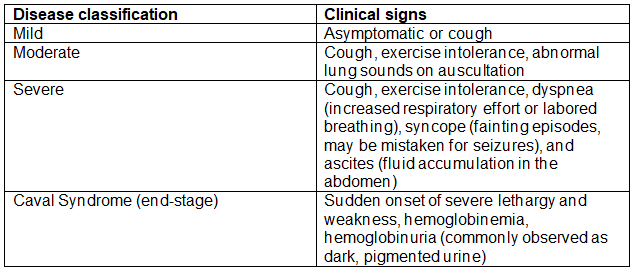
If information about the status of individual dogs is available, cases with mild heartworm disease based on clinical signs are preferred candidates for transport and efficient treatment protocols, as they are less likely to develop complications. Classification of clinical signs is outlined in the table below.
Obtaining a full clinical picture of all dogs prior to transfer may not be a realistic expectation to place on many sending shelters (i.e., requiring pulmonary auscultation by a veterinarian prior to selection for transport), but attempts can be made to select for patients less likely to have late-stage disease. Ideal candidates are younger (2-3 years or less) and are not notably demonstrating signs of severe disease to shelter staff. Older dogs may often be only mildly affected, but in endemic areas, long-standing or repeat infections are more likely, particularly without a history of past administration of heartworm preventatives.
It should be noted that cough associated with heartworm disease may look similar to a cough resulting from canine infectious respiratory disease (CIRD, aka “kennel cough”) and determining the inciting cause may not be possible. Ideally, dogs with CIRD are not transported on a vehicle with other dogs, however, so attempts should be made to rule out CIRD as a cause prior to transfer. (Have a holding period to allow the disease to run its course and for the dog to recover, providing treatment with antibiotic therapy if indicated.)
Transport considerations
Transport to a receiving partner may be an individual dog’s only option for lifesaving treatment, and transport of heartworm-positive dogs for treatment elsewhere is often an integral part of a shelter’s comprehensive lifesaving strategy. When possible, however, both sending and receiving shelters should make attempts to minimize the risk of transmission associated with relocating dogs. Because adult heartworms are not the directly transmissible life stage, this can be achieved even when transporting positive dogs. Specific testing for microfilaria (the transmissible stage) is often not possible for sending shelters, so dogs should be handled as if they can transmit microfilaria.
Choose one of these three options to prevent transmission:
1. Apply a moxidectin product (e.g., Advantage Multi); a single dose will eliminate most microfilaria.
OR
2. Administer a macrocyclic lactone preventative (e.g., Heartgard) WITH a topical canine insecticide labeled to kill and repel mosquitoes (e.g., Advantix).
OR
3. Administer a macrocyclic lactone preventative WITH a dose of isoxazoline insecticidal product (e.g., Nexgard). The isoxazoline will kill mosquitoes after they feed.
If one of these is not possible prior to transport, then one of these options should be administered as soon as possible upon arrival. The AHS provides more details:
AHS Minimizing Heartworm Transmission in Relocated Dogs
Because heartworm disease is endemic in areas of the country where other infectious disease is often prevalent (distemper, parvo), additional strategies to mitigate the risk of infectious disease during transport should be employed. For more information, see this playbook.
Diagnostics
The greater the number of worms killed during treatment, the more significant the potential for complications. However, no test or combination of tests can accurately determine the number of worms present in an individual dog. The AHS states, “It is probable that treating in the absence of diagnostics, while not ideal, is better than refusing to perform a needed treatment.”
For dogs exhibiting signs of severe heartworm disease, diagnostics may provide additional prognostic information, but even in those cases, the necessary treatment plan is the same. Vast numbers of heartworm adulticide treatments have been performed without the benefit of extensive diagnostic testing in shelters and private clinics across the country. In an effort to extend limited resources to save the most lives possible, it is reasonable to forgo extensive pre-treatment diagnostic testing so that we may treat more dogs suffering from heartworm disease.
Pre-injection medications
Doxycycline, an antibiotic, has efficacy against Wolbachia organisms, a symbiotic bacteria harbored inside heartworms; eliminating the Wolbachia weakens adult worms. Dogs treated with doxycycline have less pulmonary pathology associated with the death of worms during treatment. Doxycycline also prevents larval stages of heartworms from developing into adults and will reduce microfilaria (the stage that is transmitted to other dogs via mosquito).
Doxycycline is given at 10mg/kg twice daily for four weeks prior to melarsomine injections. This can be completed at any point prior to injections, and some time between completion of doxycycline and melarsomine injections is preferred (though not mandatory in mild infections). Alternative options to reduce medication administration time (which have not been evaluated for efficacy but are commonly employed in shelters) include once-daily doxycycline administration or reducing the duration of administration to two weeks instead of four. These are also options for dogs who cannot tolerate the twice-daily high dose due to gastrointestinal upset.
Heartworm prevention should be administered for 60 days prior to melarsomine injections. Macrocyclic lactone preventives eliminate larval-stage heartworms, and melarsomine kills adult worms, but neither are effective against juvenile worm stages. Beginning a preventative will keep any new infections from occurring, and the waiting period (described below) will allow juveniles to mature into adults, so melarsomine will be effective against those newly matured adults. In practice, this usually means melarsomine is first administered at approximately the same time that the dog receives the third dose of monthly preventive.
Melarsomine injections
Melarsomine is administered via deep intramuscular injection in the lumbar epaxial muscles at a dose of 2.5mg/kg. The first injection is given 60 days (or longer) after the first dose of heartworm prevention. The second injection is given four weeks after the first, and the final (third) injection is given the following day on the opposite side (right vs. left) of the second injection.
Prednisone is dispensed following the first injection at 0.5mg/kg twice daily for seven days, then once daily for seven days, then every other day for seven doses. This course is repeated at the time of the second injection. Prednisone is a steroid and reduces inflammation caused by dying worms, so it reduces the risk of post-treatment complications.
Many dogs experience pain following melarsomine injections, so providing preemptive pain control is recommended. Gabapentin is a good choice, given at 10-20mg/kg twice daily. Administration can begin the morning of the melarsomine injection, so that the administration of injectable pain medication is not required at the injection visit.
Melarsomine products require reconstitution of the powder component with a provided diluent prior to administration. Once reconstituted, it must be used within one day (24
hours). To avoid waste and be as cost-efficient as possible, it is prudent to schedule multiple dogs on the same day for injections. The same reconstituted vial may be used for dogs receiving injections on two consecutive days (approximately 24 hours apart), but it must be refrigerated when not in use. Click here for more information on giving deep epaxial injections.
Alternative injection protocol
The previously accepted two-injection melarsomine protocol (two injections given 24 hours apart) has 90% efficacy, meaning that it kills 90% of worms, which is notably different than completely clearing that percentage of dogs of all worms. Efficacy for individual dogs and complete worm clearance is considerably lower. The three-injection protocol has 98% efficacy and a decreased risk of complications.
A two-injection protocol shortens the length of stay of the dog in care by about four weeks (and the associated activity restriction) and is less expensive in terms of materials. However, the benefits of the three-injection protocol outweigh those risks in most cases, and by housing dogs in foster care, adverse effects of longer stays in care can be avoided. Shelters may consider this option, however, as long as the risks are understood and the benefits outweigh those risks for their particular situation or individual patient.
Housing and activity restriction
Strict activity restriction should begin at the time of the first injection and should continue for 4-6 weeks after each injection. (Four weeks is typically acceptable for asymptomatic dogs; longer restriction is ideal for dogs demonstrating significant clinical signs associated with heartworm disease.)
If injections are given on schedule (four weeks apart between the first and second), this means 8-10 weeks of strict restriction. Ideally, the dog is housed in a foster or adoptive home during this period so that he/she can be monitored more closely and can receive the mental stimulation and enrichment that isn’t possible in a shelter environment during the restriction period.
Various models exist for treatment and follow-up while in foster care or after adoption. If an adopter is not immediately available, fostering a heartworm-positive dog undergoing treatment is appealing to many foster volunteers, as the timeline is well-defined and, by necessity, even large active dogs must be restricted. Some organizations prefer to keep dogs under the ownership of the organization, even if the foster caregiver plans to adopt, so that the organization maintains control over medical decision-making. Others finalize the adoption and coordinate treatment appointments at the shelter or with a partner clinic.
To facilitate activity restriction, trazodone is a good choice for very active dogs who are not responding well to crate restriction. Adopters and foster caregivers should be given tools and ideas for providing enrichment.
Follow-up diagnostic testing
Follow-up testing information should be provided to adopters and, ideally, follow-up should be performed at their vet’s. It takes several weeks or months for dead heartworms to break down, so recently treated dogs will still test positive for an extended period following treatment, even though no live worms are present.
Some dogs will test negative within 3-6 months after treatment; some may remain positive longer. If a dog tests positive earlier than nine months, do not re-treat; test at nine months.
For dogs who still test positive at nine months post-treatment, ensure heartworm prevention compliance. (Treatment failures with the three-injection protocol are uncommon; re-infection can occur if prevention is not maintained.) If treatment failure is suspected, consider re-treating with two melarsomine injections, 24 hours apart.
Sample Procedure and Program Information Documents
Now that you have a general understanding of what a shelter heartworm management program looks like, the following documents can act as templates or inspiration as you implement or scale up your own program. Using the considerations and program composition notes above, you should use the following as guidelines or building blocks when creating your own standard operating procedures or documents (both internal and public). If you need further assistance or clarification, please reach out to your regional strategist, regional director, or the Best Friends national shelter support team at team2025@bestfriends.org.
- Sample Heartworm Treatment Protocol
- Heartworm Treatment Dose Charts
- Supply List
- Treatment Schedule (Fillable) for Foster Volunteers and Adopters
- List of Additional Resources and Links
Updated May 2022
If you found this manual helpful, you find our complete catalog of manuals, handbooks, and playbooks here.